

Glucose
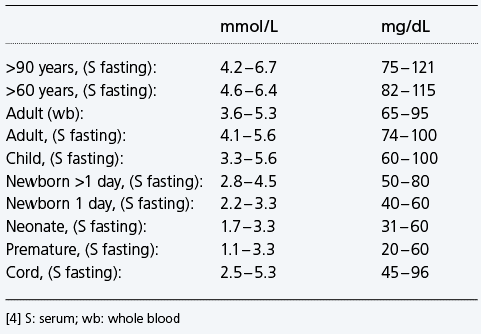
Reference interval glucose - examples
Physiological significance of glucose and blood glucose regulation
Why measure blood/plasma glucose ?
When should glucose be measured ?
Hyperglycemia and diabetes
Hyperglycemia and the critically ill patients
Causes of hyperglycemia
Symptoms of hyperglycemia
Hypoglycemia
Causes of hypoglycemia
Symptoms of hypoglycemia
Hypoglycemia and neonates
Causes of hypoglycemia in neonates include
Glucose, the most abundant carbohydrate in human metabolism, serves as the major intracellular energy source (see lactate). Glucose is derived principally from dietary carbohydrate, but it is also produced – primarily in the liver and kidneys – via the anabolic process of gluconeogenesis, and from the breakdown of glycogen (glycogenolysis). This endogenously produced glucose helps keep blood glucose concentration within normal limits, when dietary-derived glucose is not available, e.g. between meals or during periods of starvation.
Reference interval glucose – examples
Physiological significance of glucose and blood glucose regulation
The body can only utilize glucose within cells, where it is the major source of energy. In every cell of the body this energy is released by the oxidation of glucose to carbon dioxide and water in two sequential metabolic pathways: the glycolytic pathway and the citric acid cycle. During this oxidative process the energy-rich compound adenosine triphosphate (ATP) is formed, and this, in turn, drives the multiplicity of chemical reactions required for tissue cells to remain viable and fulfill their function. Oxidation of one molecule of glucose by this process yields 36 molecules of energy-rich ATP (Fig. 15).
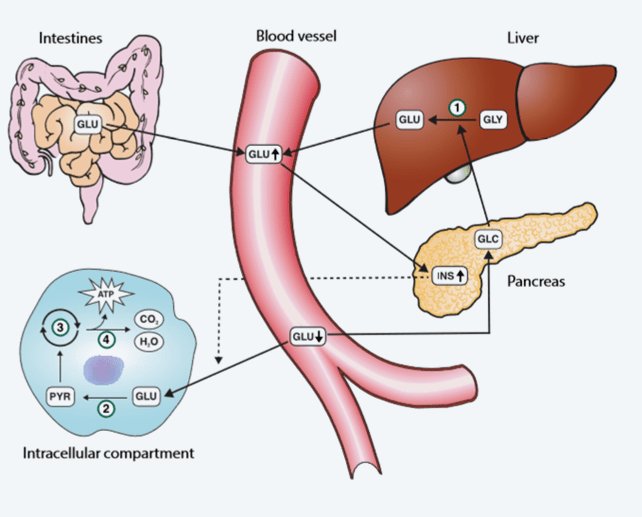
FIG. 15: The glucose pathway. 1: Glycogenolysis; 2: Glycolysis; 3: Citric acid cycle; 4: Oxidative phosphorylation GLU: Glucose; GLY: Glycogen; GLC: Glucagon; INS: Insulin; PYR: Pyruvate; ATP: Adenosine triphosphate
For this energy-generating function to proceed, glucose must be transported from the intestines (food) or liver (gluconeogenesis, glycogenesis) to body cells via the blood circulation, and enter the tissue cells. Glucose entry to cells from blood is dependent on insulin. This, in part, explains why hyperglycemia is a defining feature of diabetes and highlights the role of insulin in regulating blood glucose concentration. The maintenance of blood glucose concentration within normal limits is in fact dependent on two pancreatic hormones: insulin and glucagon. Insulin is secreted from the pancreas in response to rising blood glucose, and has the effect of reducing blood glucose; whereas glucagon is secreted from the pancreas in response to falling blood glucose and has the effect of increasing blood glucose. By the synergistic opposing action of these two hormones, blood glucose concentration remains within normal limits.
Insulin reduces blood glucose by:
- Enabling entry of glucose to cells from blood
- Promoting cell metabolism (oxidation) of glucose via the glycolytic pathway
- Promoting formation of glycogen from glucose in the liver and muscle cells
- Inhibiting liver/kidney production of glucose via gluconeogenesis
Glucagon increases blood glucose by:
- Promoting liver/muscle production of glucose from glycogen (glycogenolysis)
- Promoting liver/kidney production of glucose from non-carbohydrate sources (gluconeogenesis)
In situations where there is reduced carbohydrate supply from the intestines, gluconeogenesis becomes particularly important for maintaining a normal blood glucose level and thereby the supply of glucose to all tissues [151].
The non-carbohydrate substrates from which glucose is formed during gluconeogenesis include:
- Proteins
- Glycerol
- Glucose metabolism intermediaries like lactate and pyruvate [152]
Despite widely variable intervals between meals or the occasional consumption of meals with a substantial carbohydrate load, blood glucose concentration does not usually rise above around 8.0 – 9.0 mmol/L (144 – 162 mg/dL) nor fall below around 3.5 mmol/L (63 mg/dL) in healthy individuals [153]. The highest levels (8.0 – 9.0 mmol/L) occur 1 – 1.5 hours after eating carbohydrate-containing food and the lowest levels occur before food in the morning (i.e. after an overnight fast).
Why measure blood/plasma glucose?
The principal reason for measuring circulating glucose concentration is to diagnose and monitor diabetes mellitus, a very common chronic metabolic condition characterized by increased blood glucose concentration (hyperglycemia), due to an absolute or relative deficiency of the pancreatic hormone insulin [148]. The two main types of diabetes are referred to as type 1 (insulin-dependent) and type 2 (insulin-resistant). Diabetes treatment, which is aimed at normalizing blood glucose concentration, is associated with constant risk of reduced blood glucose (hypoglycemia), which can lead to impaired cerebral function, impaired cardiac performance, muscle weakness, and is associated with glycogen depletion and diminished glucose production.
Abnormality in blood glucose concentration is not confined to those with diabetes. Transient (stress-related) hyperglycemia is a common acute effect of critical illness, whatever its cause. Identification and effective treatment of hyperglycemia (i.e. normalizing blood glucose) improves the chances of surviving critical illness for both diabetic and non-diabetic patients [149].
Neonates, particularly those born prematurely, are at high risk of reduced blood glucose (hypoglycemia). According to [150] the key to prevent complications from glucose deficiency “is to identify infants at risk, promote early and frequent feedings, normalize glucose homeostasis, measure glucose concentrations early and frequently in infants at risk, and treat promptly when glucose deficiency is marked and symptomatic” [150].
When should glucose be measured?
When there are signs and symptoms of hypoglycemia, suspicion of diabetes (hyperglycemia), or hyperglycemia as result of stress in critically ill patients [154].
Hyperglycemia and diabetes
In the absence of critical illness diabetes is confirmed if fasting plasma glucose is ≥7.0 mmol/L (126 mg/dL) or random plasma glucose is consistently ≥11 mmol/L (>198 mg/dL). Those with fasting plasma glucose in the range of 5.6 – 6.9 mmol/L (101 – 124 mg/dL) have fasting hyperglycemia, but it is not sufficiently severe to make the diagnosis of diabetes. The label ”impaired fasting glucose” is applied to these individuals, who are at much greater-than-normal risk of developing diabetes at some time in the future. The acute and chronic long-term complications of diabetes are avoided by normalization of blood glucose concentration using exogenous insulin and/or other blood glucose-lowering drugs. Recommended targets are for preprandial (fasting) plasma glucose to be maintained in the range of 3.9 – 7.2 mmol/L (70 – 130 mg/dL), and peak (1 – 2 hours postprandial) plasma glucose should not exceed 10.0 mmol/L (180 mg/dL) [155].
Hyperglycemia and the critically ill patients
Hyperglycemia occurs frequently, whether secondary to diabetes or stress-induced (in the non-diabetic), in the critically ill patient [156]. The body increases glucose production and can become resistant to the effects of insulin, with resulting hyperglycemia. In one study, intensive insulin therapy targeting arterial glucose levels of 4.4 – 6.1 mmol/L (79 – 110 mg/dL) in a primarily surgical ICU patient population resulted in a significant decrease on morbidity and mortality [154]. However, aggressive intensive insulin therapy can lead to hypoglycemia [157]. The American Diabetes Association (ADA) [155] recommends that in the majority of critically ill patients in the ICU, insulin infusion should be used to control hyperglycemia if blood glucose exceeds 10 mmol/L (180 mg/dL). The aim of such therapy is to maintain glucose in the range of 7.8 – 10 mmol/L (141 – 180 mg/dL). For selected patients more stringent goals, such as 6.1 – 7.8 mmol/L (110 – 141 mg/dL), may be appropriate as long as it does not lead to significant hypoglycemia. According to ADA a target <6.1 mmol/L (110 mg/dL) is not recommended [155].
Causes of hyperglycemia [23]
- Trauma
- Stroke/myocardial infarction
- Surgery
- Diabetes mellitus
- Acute pancreatitis
- Endocrine hyperfunction
- Hemochromatosis
- Impaired glucose tolerance/impaired fasting glucose
- Drugs
Symptoms of hyperglycemia
- Headaches
- Dehydration
- Palpitations
- Respiratory abnormalities
- Frequent urination
- Fatigue
- Weight loss
- Thirst
- Gastrointestinal disturbances
- Altered mental status and/or sympathetic nervous system stimulation
- Ketonemia/-uria
- Pseudohyponatremia
- Metabolic acidosis
Critically ill patients can experience rise in blood glucose concentration as a result of:
- The initial trauma
- Surgery
- Inhaled anesthesia
- Medications, particularly corticosteroids
- Intravenous solutions used for drug and fluid administration
- Dialysis solutions
- Infections, particularly sepsis
Hypoglycemia
Hypoglycemia is defined as decreased blood glucose concentration. The glucose level at which an individual becomes symptomatic is highly variable; therefore a single blood glucose concentration that categorically defines hypoglycemia is not established [158]. In some intensive care settings hypoglycemia is defined as blood glucose <2.2 mmol/L (40 mg/dL) [156].
Causes of hypoglycemia [23]
- Diabetes treatment (most common cause)
- Insulinoma, liver disease
- Postgastrectomy
- Insulin abuse
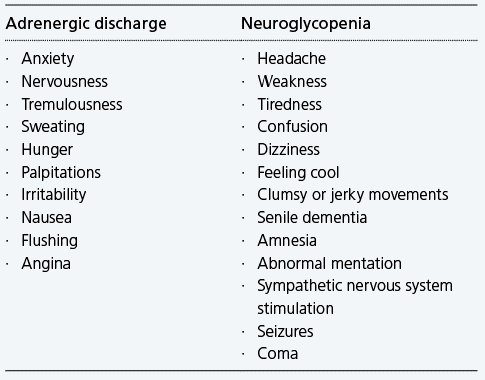
Symptoms of hypoglycemia
Hypoglycemia symptoms can either result from adrenergic discharge or from neuroglycopenia.
Hypoglycemia and neonates
In neonates, hypoglycemia is a common metabolic issue. However, there is no consensus on a single blood glucose concentration that defines hypoglycemia in this population. Experts agree that the neurological disabilities associated with neonatal hypoglycemia depend on gestational and chronological age and associated risk factors such as hypoxic-ischemic encephalopathy and that they frequently result after situations of persistent and severe hypoglycemia [159,160].
Although there is no consensus, most expert authors support the cut-off value of 2 mmol/L (36 mg/dL) for asymptomatic healthy newborns. Values down to 1.7 mmol/L (31 mg/dL) have been suggested in an otherwise healthy term infant [161]. Operational thresholds <2.2 mmol/L (<40 mg/dL) during the first 24 hours and <2.8 mmol/L (<50 mg/dL) thereafter are also suggested [162]. Many neonate units aim to maintain blood glucose levels above 2 – 3 mmol/L (26 – 54 mg/dL) and below 10 – 15 mmol/L (180 – 270 mg/dL) in low-birth-weight or sick babies [163].
Causes of hypoglycemia in neonates include [164]:
- Inappropriate changes in hormone secretion
- Inadequate substrate reserve in the form of hepatic glycogen
- Inadequate muscle stores as a source of amino acids for gluconeogenesis
- Inadequate lipid stores for the release of fatty acids
Radiometer is using Microsoft AZURE Active Directory to authenticate users
Radiometer uses Azure AD to provide our customers and partners secure access to documents, resources, and other services on our customer portal.
If your organization is already using Azure AD you can use the same credentials to access Radiometer's customer portal.
Key benefits
- Allow the use of existing Active Directory credentials
- Single-sign on experience
- Use same credentials to access future services
Request access
You will receive an invitation to access our services via e-mail when your request has been approved.
When you accept the invitation, and your organization is already using AZURE AD, you can use the same credentials to access Radiometer's customer portal. Otherwise, a one-time password will be sent via e-mail to sign in.